Immediate implants with immediate restorations: A patient-preferred approach
Immediate implants with same-day restorations are among the most discussed topics in implant dentistry today, and for good reason.

Dr. Suzanne Caudry
Periodontist
Table of contents
Share
Background
Immediate implants with same-day restorations are among the most discussed topics in implant dentistry today, and for good reason. Patients strongly prefer avoiding a removable prosthesis during healing, making this approach increasingly in demand. When handled appropriately, immediate implants can achieve the same long-term success rates as traditionally placed implants. That said, this is one of the more technically demanding treatment plans in our field, and a few key principles guide a successful outcome.
Early results are not a reliable indicator of long-term success
Recession can continue to develop up to 18 months postoperatively or longer, which means short-term aesthetics can be misleading. Adequate bone support is essential, as soft tissue follows bone. Correct implant placement with sufficient buccal bone is critical to achieving lasting aesthetic results.
Thin tissue biotypes require additional care
Patients with thin tissue biotypes require extra attention throughout the process. In these cases, connective tissue grafting significantly improves the final outcome and is strongly recommended.
Hygiene protocol following implant restoration
For patients who have received a new dental implant, we recommend hygiene visits every 3 to 4 months for the first two years following restoration. After that, maintenance frequency can be adjusted based on each patient's oral hygiene status and individual needs.
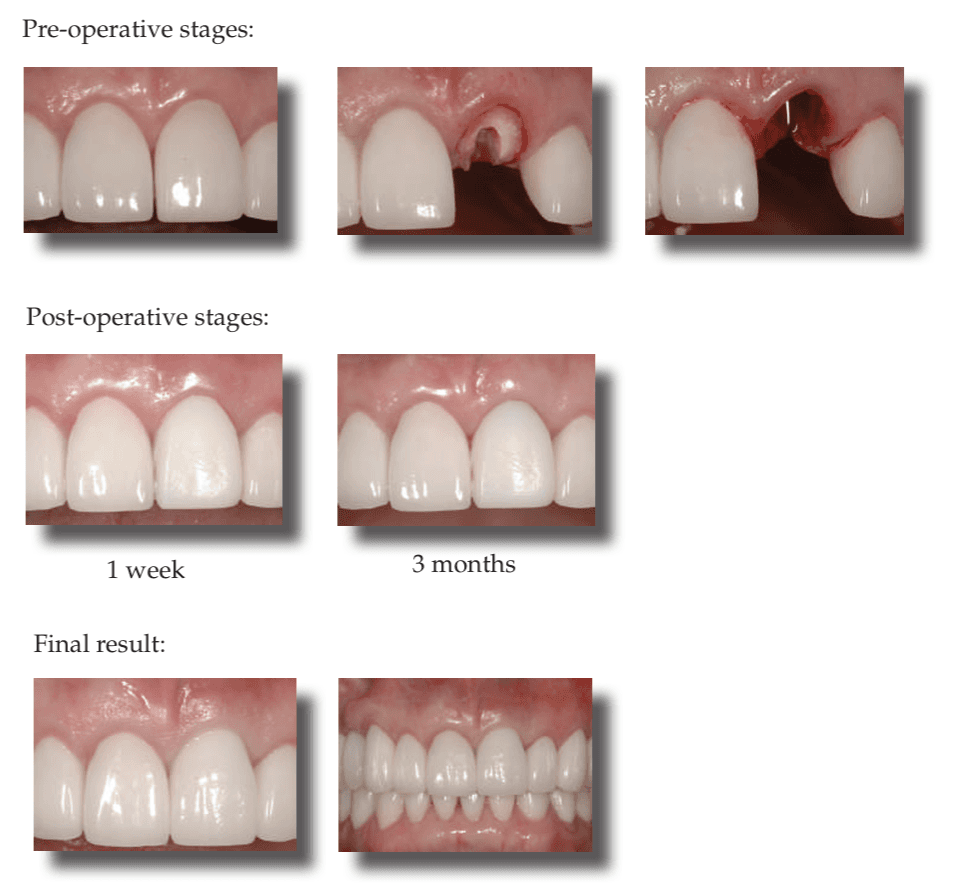
Replicating Natural Teeth With Immediate Implants
Based on the angulation and structure of the anterior maxilla, ideal implant placement for a central is not through the cingulum but rather along the axial.
Screw-retained temporaries have been preferred for this type of situation for easier retrievability, however a properly positioned implant will result in the screw access through the incisal edge. A cemented temporary crown is not the best solution because it is difficult - if not impossible - to remove overflow cement and this would lead to catastrophic failure of the implant.
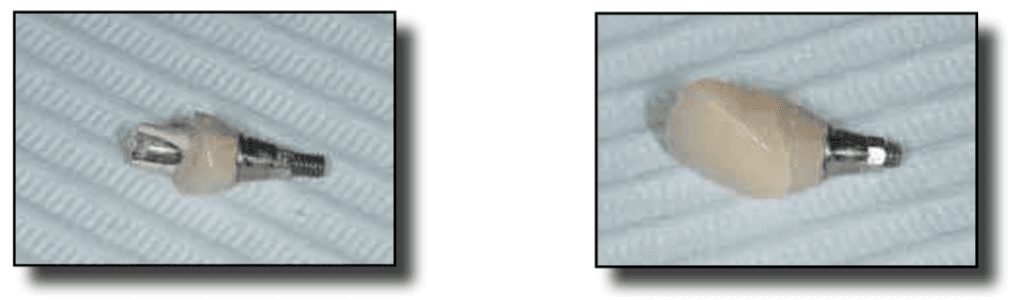
The solution: the laboratory fabricates a custom two piece temporary abutment that brings the cement line to the gingival level to facilitate cement removal. The temporary crown is cemented with temporary cement to ensure easy removal later.
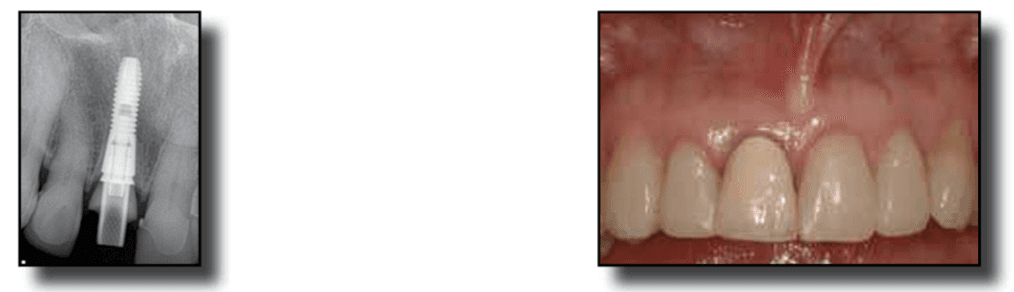
Retrieval of the crown and temporary abutment should be straightforward when the time comes for the final restoration. The result - an ideally positioned implant and perfectly sculpted soft tissue in a very challenging situation.
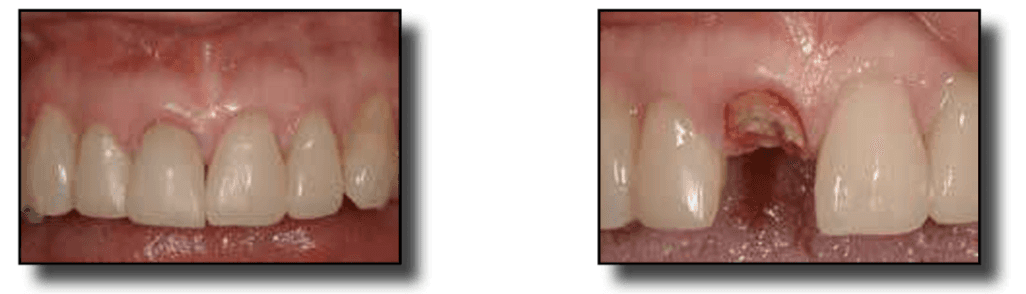
Biology May Win
Immediate implant placement continues to be a heavily debated topic and one that I have lectured on since 2005. The research has changed yet the most important question of all still remains: are the risks worth the rewards? Even the most meticulous treatment planning can be outsmarted by anatomy and biology. Anatomical issues such as bone defects and angulation can often be diagnosed pre-surgically but biological issues can be more elusive.
Minimizing surprises: pre-surgical planning
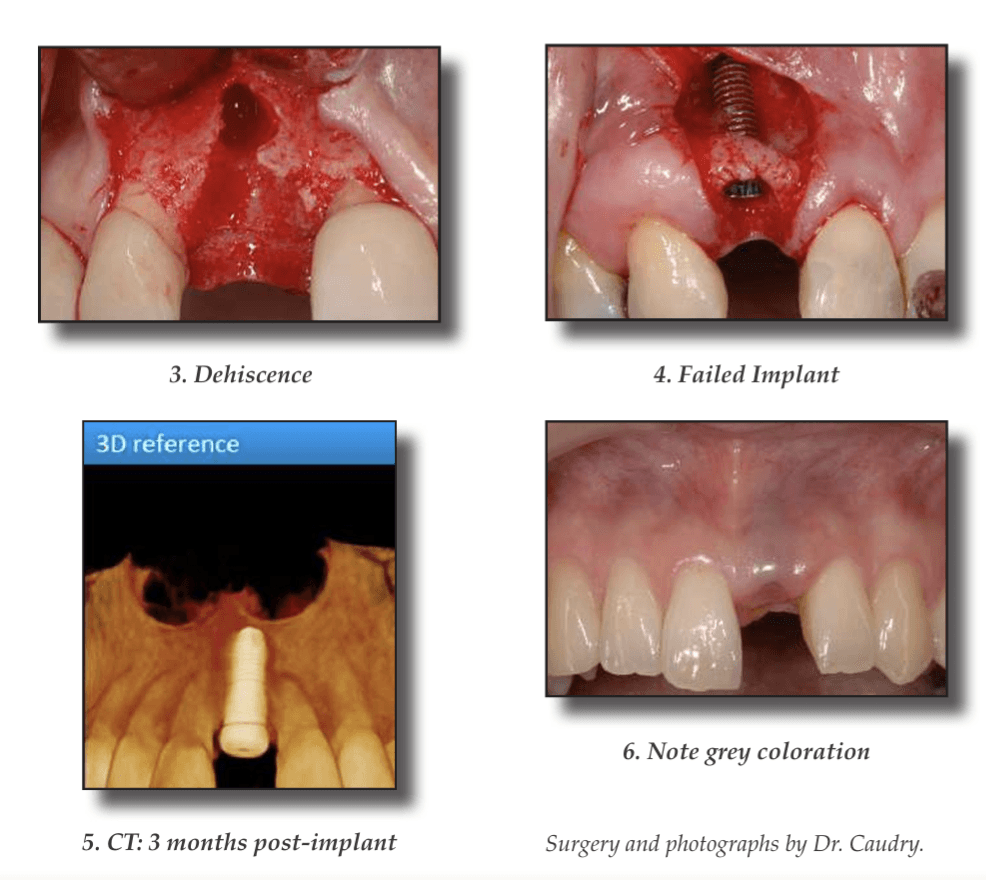
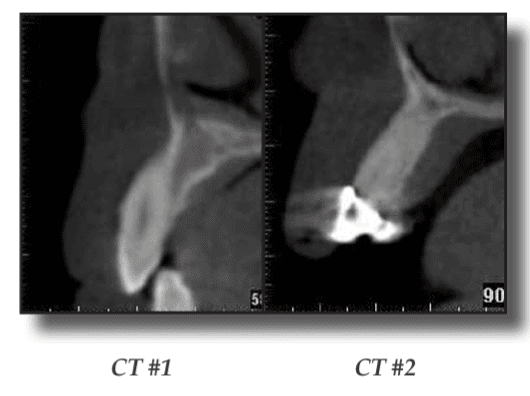
A CT scan is the best implant treatment planning tool available. CT #1 shows that there is an angulation problem, a buccal concavity and lack of bone volume. However, a CT does not always provide accurate information regarding bone thickness, or about defects such as dehiscences and fenestrations. The presence of socket walls is a critical component for successful immediate implant placement yet we will not always be sure of the status of the socket walls until after the tooth has been extracted. In CT#2 the angulation is acceptable but we can see that the natural tooth extends from the buccal to the palatal plate. After extraction, the integrity of the socket walls is questionable. Here, biology may win.
A flapless technique is preferred for immediate implants. Sounding bone alone would rule out a dehiscence (3) but it would not rule out a fenestration such as the one that likely existed before the implant was placed (4). Probing upon extraction will disclose whether socket walls exist but not the thickness of those walls. Yet again, biology may win.
The volume of bone in this case seemed sufficient at the time of immediate implant placement - however three months later, there had been significant resorption of the buccal plate (5 & 6). The Winter issue of this Newsletter will review the case in greater detail.