Temporization: Post-Surgical Planning
One of the most hotly debated areas in Implant Dentistry relates to immediate placement and immediate temporization.

Dr. Suzanne Caudry
Periodontist
Table of contents
Share
One of the most hotly debated areas in Implant Dentistry relates to immediate placement and immediate temporization. Since first lecturing on this topic more than a decade ago, I find that our scientific community is still divided on whether treatment risks outweigh potential rewards. We have yet to reach a definitive consensus.
It is critical that post-surgical treatment planning for temporization of an immediate implant be discussed with the patient prior to surgery. Patient occlusion, parafunction and compliance are also significant risk factors that must be thoroughly investigated and addressed prior to commencing treatment.
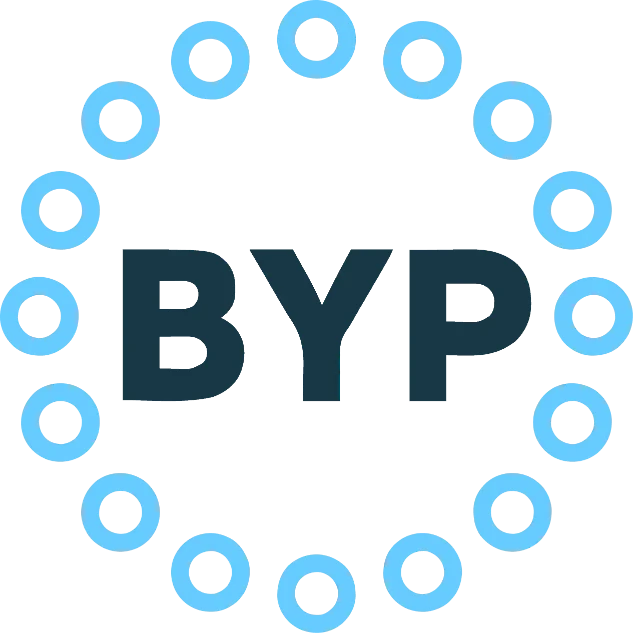
Even an appliance as seemingly straightforward as an Essix-type of retainer (Photo 1a, 1b) has the potential for risk. A question often overlooked: Will the patient tolerate this temporary solution? If so, will they be compliant regarding its limited functionality?
Temporary abutments and crowns
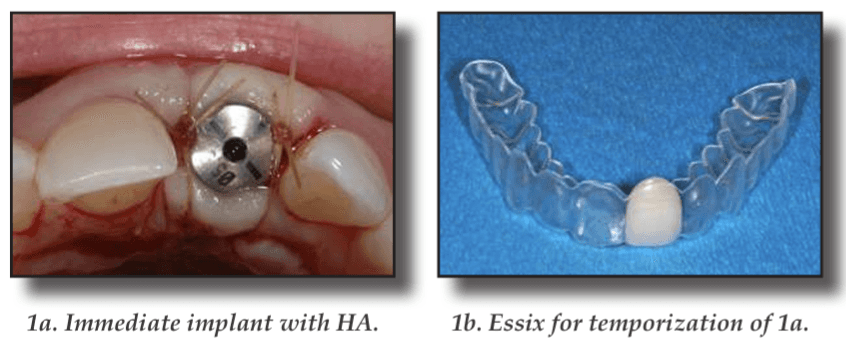
Temporary abutments and temporary crowns are the preferred method of temporization for immediate implants as they contribute to successful aesthetics in the short and long term (2). The risk factors are high and often relate directly to the patient. Does the patient fully understand the functional limitations of a temporary crown and abutment? Fracture of the temporary crown will be a nuisance but catastrophic failure of the implant is a much greater concern. (Refer to the Immediate Implants Newsletter for a guideline to replicating natural teeth with cement-retained temporaries).
Although this patient was fully informed and signed a waiver regarding the limits of functionality of the temporary, he bit into an apple shortly after surgery (3).
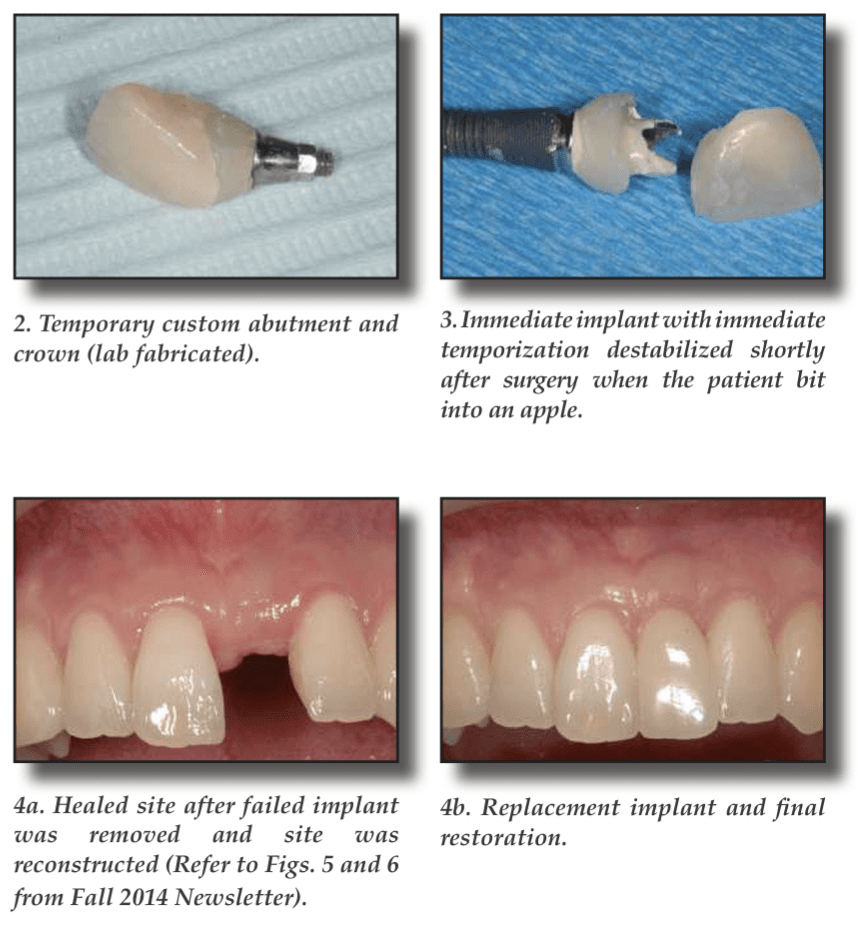
In our previous Newsletter we looked at a case with significant bone resorption at 3 months post-implant placement. Since the buccal bone fully resorbed, the implant was removed and the site was reconstructed (4a). After healing, another implant was subsequently placed. The final result is shown (4b). In this instance, the risk of placing an immediate far exceeded the reward due to the complications.